
A cough that lingers can feel like a stuck alarm. It’s not always loud, but it’s always there, during calls, in meetings, and at bedtime. If you’ve been coughing for 8 weeks or longer as an adult, it fits the definition of a chronic cough.
Three of the most common (and very treatable) explanations are allergies with postnasal drip, asthma (including cough-variant asthma), and reflux (GERD, including “silent reflux” that shows up without heartburn). The tricky part is that symptoms overlap, so guessing based on one clue often leads to frustration.
This guide walks through practical patterns that help you sort out likely chronic cough causes, and it also shows when it’s time to get evaluated so you can stop cycling through random remedies.
Start with patterns: clues in timing, triggers, and what the cough feels like
When a cough won’t quit, most people focus on the sound. A better starting point is the pattern. Think of it like tracking a smoke smell in a house: you’re looking for when it’s strongest, what sets it off, and what else is happening in the background.
When does it happen most?
- Night cough can point toward asthma (airways tend to tighten at night), reflux (more exposure when lying down), or postnasal drip that pools when you’re flat.
- Morning cough often shows up with postnasal drip or reflux-related throat irritation (some people wake up hoarse or need to clear their throat for the first hour).
- All-day cough can happen with any cause, but it often suggests constant exposure (dust, smoke, workplace irritants) or more than one trigger.
What seems to set it off?
Pay attention to repeatable triggers:
- Exercise, cold air, viral colds, and strong scents: think asthma or reactive airways.
- Meals, late-night snacks, bending over, alcohol: think reflux.
- Seasons, pets, dusty rooms, damp spaces: think allergies.
What comes along with the cough?
The “side symptoms” can be more useful than the cough itself:
- Runny or stuffy nose, itchy eyes, and frequent throat clearing often travel with allergies.
- Chest tightness, wheezing, and shortness of breath lean toward asthma (but wheezing can be absent in cough-variant asthma).
- Hoarseness, a lump-in-throat feeling, and a and sour taste can point toward reflux, including silent reflux.
The goal isn’t to self-diagnose. It’s to notice enough detail that you and your clinician can move faster.
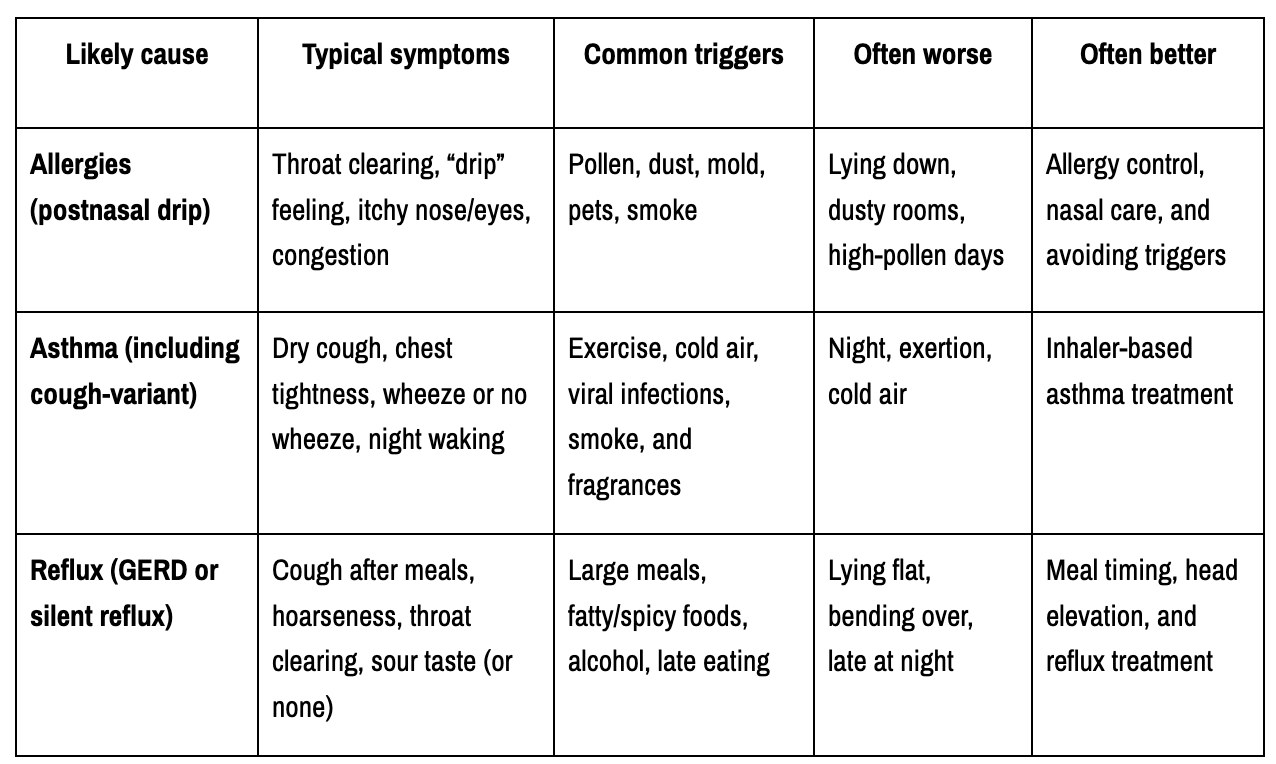
Quick comparison: allergies vs asthma vs reflux (the easy-to-remember differences)
Here’s a plain-language snapshot you can come back to.
For a deeper medical overview of common causes and treatments, see Cleveland Clinic’s chronic cough guide.
The overlap problem: when you might have more than one cause
Real life rarely fits in one box. It’s common to have two (or even three) drivers at once.
Postnasal drip can irritate the throat and keep the cough reflex “on,” even when your lungs are fine. Reflux can inflame the throat and voice box and also worsen asthma symptoms. Poor sleep and stress can lower your cough threshold, so you cough more from the same trigger.
Newer clinical thinking also highlights a “treatable traits” approach: instead of forcing one diagnosis, clinicians look for the specific factors keeping your cough going (nasal inflammation, asthma, reflux, medication side effects, irritant exposure, or cough hypersensitivity) and address them step-by-step.
That step-by-step part matters. If you change five things at once, you won’t know what actually helped.
Allergy-related cough: when mucus drips and irritation are the main drivers
Allergy cough is often less about the lungs and more about what’s happening above them. Allergens (like pollen or dust mites) inflame the lining of the nose and sinuses. Your body makes extra mucus, and that mucus can drip down the back of the throat. The throat gets irritated, and the cough reflex keeps firing, like a faucet that won’t stop dripping.

Photo by Vlada Karpovich
Triggers can be seasonal or indoor:
- Seasonal: tree, grass, or weed pollen.
- Indoor: dust mites, mold, pet dander, smoke, and strong odors.
If you’re mostly fine outdoors but cough more at home, think about bedroom exposures (pillows, carpeting, humidity, pets sleeping in the room). If you’re fine at home but cough at work, consider fragrance policies, dust, chemicals, or poor ventilation.
Signs it leans allergy: throat clearing, itchy nose, and cough that tracks with seasons
Allergy-related cough often comes with a cluster of upper-airway symptoms:
- Frequent throat clearing
- A tickle in the throat or a “drip” sensation
- Itchy nose, sneezing, watery eyes
- Nasal congestion or pressure
What’s often absent: true chest tightness, wheezing, or shortness of breath (though people can have allergies and asthma together).
A simple tracking tip: jot down your cough severity (0 to 10) next to exposures. Note high-pollen days, time spent cleaning, being around pets, or being in a musty space. The pattern often shows itself within 2 weeks.
For a practical, patient-friendly explanation of allergy cough, see ACAAI’s overview of cough and allergies.
What helps and what to ask your clinician about
Treatment usually works best when it’s layered, starting with the lowest-risk steps:
Trigger reduction: washing bedding in hot water, managing indoor humidity, HEPA filtration, smoke avoidance, and keeping pets out of the bedroom if you’re sensitive.
Nasal care: saline rinses can reduce mucus and irritants. Many people notice less throat clearing once the nose is calmer.
Medications to discuss: clinicians often start with antihistamines and/or nasal steroid sprays, depending on symptoms and medical history. Allergy testing can help if triggers are unclear or symptoms keep returning.
Immunotherapy (allergy shots): sometimes considered when symptoms are persistent, clearly allergy-driven, and not controlled with routine steps.
One caution: over-the-counter decongestant nasal sprays can cause rebound congestion if used too long. If you feel dependent on a spray, that’s a good reason to check in with a clinician.
Asthma cough, including cough-variant asthma: when the lungs are extra reactive
Asthma isn’t just “wheezing.” It’s ongoing inflammation in the airways that makes them sensitive. When triggered, the airway lining swells, muscles tighten, and mucus can increase. The result can be coughing, wheezing, chest tightness, or shortness of breath.
In cough-variant asthma, cough is the main symptom. People may never hear a wheeze. They may just feel like they can’t shake a dry cough that flares with triggers.
Common triggers include:
- Exercise
- Cold air
- Smoke or vaping exposure
- Viral infections (a cold that “turns into” a long cough)
- Strong scents and cleaning products
Signs it leans to asthma: cough with exercise, cold air, or at night
Asthma cough often follows a recognizable script:
- Cough that starts or worsens during exercise or right after
- Cough that’s worse in cold air
- Nighttime cough, sometimes waking you up
- Chest tightness or a “can’t get a deep breath” feeling
- Personal or family history of asthma, eczema, or allergies
In kids, asthma may show up mainly as a lingering cough, especially after colds. In adults, cough-variant asthma can be overlooked because the classic wheeze isn’t there.
If your cough reliably spikes after a brisk walk in cold weather, that pattern is worth bringing up. It’s one of the more helpful clues.
How asthma is checked and treated (without guessing)
A good evaluation usually includes spirometry, a breathing test that measures airflow. Some people need additional testing if spirometry is normal, but symptoms still fit asthma.
Treatment is aimed at reducing airway inflammation, not just quieting the cough for a day.
In plain terms:
- A rescue inhaler relaxes airway muscles fast for short-term relief.
- A controller medication (often an inhaled steroid) reduces inflammation over time to prevent flares.
If you start asthma treatment, follow-up matters. If symptoms don’t improve, the plan should be adjusted, or another cause should be considered.
For a helpful breakdown of how asthma, a runny nose, and reflux can all mimic each other, see University Hospitals’ chronic coughing article.
Reflux and “silent reflux”: when the throat is reacting to stomach contents
Reflux isn’t only heartburn. Stomach contents can move upward, especially after meals or when lying down. Sometimes that reflux irritates the esophagus (classic GERD). Other times it irritates the throat and voice box more than the chest, which can look like a cough, hoarseness, and constant throat clearing.
This is why “silent reflux” can be confusing. There may be no burning at all, just a throat that feels inflamed.
Clues can include:
- Hoarse voice, especially in the morning
- A lump-in-throat feeling
- Frequent throat clearing
- A cough that’s worse after eating, laughing, or talking a lot
Signs it leans reflux: worse after meals, bending over, or lying flat
Reflux cough often follows gravity and timing:
- Worse after larger meals
- Worse after spicy or fatty foods
- Worse with alcohol (even a modest amount for some people)
- Worse when bending over (loading the dishwasher can be a weirdly reliable trigger)
- Worse, lying flat, with coughing fits at night
- Morning hoarseness or a scratchy throat
Late dinners matter. If you eat at 9 pm and fall asleep at 10 pm, your throat may get bathed in reflux for hours. You might not feel heartburn, but your cough will.
What usually helps: meal timing, sleep position, and medical options to discuss
Reflux care often starts with practical steps that reduce exposure:
Meal timing: finishing dinner earlier and avoiding heavy bedtime snacks can reduce nighttime symptoms.
Portion size: smaller meals create less pressure and less reflux.
Sleep position: elevating the head of the bed can help. Extra pillows often bend the neck but don’t lift the torso enough, so a wedge or bed risers may work better for some people.
Food patterns: identify your personal triggers. For many, fatty foods, chocolate, peppermint, and acidic drinks are common offenders, but it varies.
Clinicians may also recommend a time-limited trial of medications (such as antacids, H2 blockers, or PPIs) based on your symptoms and history, and they’ll reassess your response rather than leaving you on autopilot.
When to get checked sooner, and what a step-by-step workup can look like
Most chronic coughs are treatable, but they deserve a plan. A structured evaluation can prevent months of trial and error.
A typical stepwise approach may include:
- A careful history (timing, triggers, associated symptoms)
- Review of medications (ACE inhibitors are a classic cause of chronic cough)
- Smoking and vaping review, plus secondhand exposure
- Consideration of post-viral cough (common after respiratory infections)
- A chest X-ray is indicated, especially if symptoms are persistent or atypical
- Targeted testing or treatment trials for allergies, asthma, and reflux
If you want a clinician-facing framework for how chronic cough is evaluated, University of Iowa’s chronic cough evaluation resource outlines a clear differential and workup mindset.
For people who prefer to start with a thorough, whole-person review (symptoms, lifestyle, exposures, and medical history), a structured telehealth visit can be a strong first step. Transformational Life Consulting offers telehealth allergy and immunology services led by Dr. Deepa Grandon, a triple board-certified physician with 23-plus years of experience.
Red flags: symptoms that should not wait
Seek prompt medical care if you notice:
- Coughing up blood
- Unexplained weight loss
- Fever that persists
- Chest pain
- Severe shortness of breath
- Repeated pneumonia or frequent lung infections
- Choking episodes or concern for aspiration
- New cough in a smoker over 40
- Cough lasting beyond 8 weeks without a clear plan or follow-up
These don’t automatically mean something dangerous is happening, but they do mean you shouldn’t wait it out alone.
Prepare for your visit: the simple notes that speed up answers
A few notes can save time and help your clinician connect the dots:
- Start date (or best estimate)
- Day vs night pattern
- Relation to meals, exercise, and lying down
- Seasonal changes and indoor triggers (pets, damp basement, new carpet, workplace scents)
- Medications and what you tried, plus what changed (better, worse, no effect)
- Any reflux signs (hoarseness, sour taste, lump feeling)
- Any allergy signs (itchy nose, sneezing, watery eyes)
- Any asthma cues (night cough, cold-air cough, chest tightness)
Bring your questions, too. You deserve clarity, not a shrug and another bottle of cough syrup.
Key Takeaways
- A chronic cough usually has a reason, even when it feels mysterious.
- Allergies often come with a drip and throat irritation.
- Asthma is often tied to triggers like cold air or exercise (and cough can be the main symptom), and reflux often follows meals and lying down, including silent reflux without heartburn.
- Overlap is common, so a step-by-step plan beats guessing.
If your cough has become part of your daily routine, treat that as useful information, not a personal failure. With a structured evaluation and targeted care, most people can get real relief and get their voice and sleep back. The next best step is simple: write down your pattern and ask for a plan that addresses the likely cause, not just the noise.
Stay connected with news and updates!
Join our mailing list to receive the latest news and updates from our team.
Don't worry, your information will not be shared.
We hate SPAM. We will never sell your information, for any reason.